Δημοσίευση άρθρου των ιατρών του Heart Center στο κορυφαίο καρδιολογικό έντυπο JACC- Cardiovascular Interventions του American College of Cardiology Foundation, με θέμα «An Unexplained Cause of Oxygen Desaturation Following Heterotopic Tricuspid Valve Replacement». Δημοσίευση, 8 Απριλίου 2024.
—
A 72-year-old woman with mitral valve replacement performed 5 years prior, diabetes mellitus, severe chronic renal impairment, and persistent atrial fibrillation suffered from advanced right heart failure (NYHA functional class IV), requiring recurrent admissions for intravenous diuretics. Of note, her pro–B-type natriuretic peptide levels were 4,661 pg/mL.
Echocardiography revealed a normally functioning metallic mitral valve but torrential tricuspid regurgitation. The tricuspid valve anatomy was deemed unsuitable for TriClip (Abbott) intervention because of a large coaptation gap, leaflet tethering, and acoustic shadowing caused by the mitral prosthesis. Because of the high surgical risk (EuroSCORE II of 15.49%, TRI-SCORE of 22%), the decision was made to proceed with heterotopic tricuspid valve replacement using the TricValve (P+F Products + Features GmbH) system.
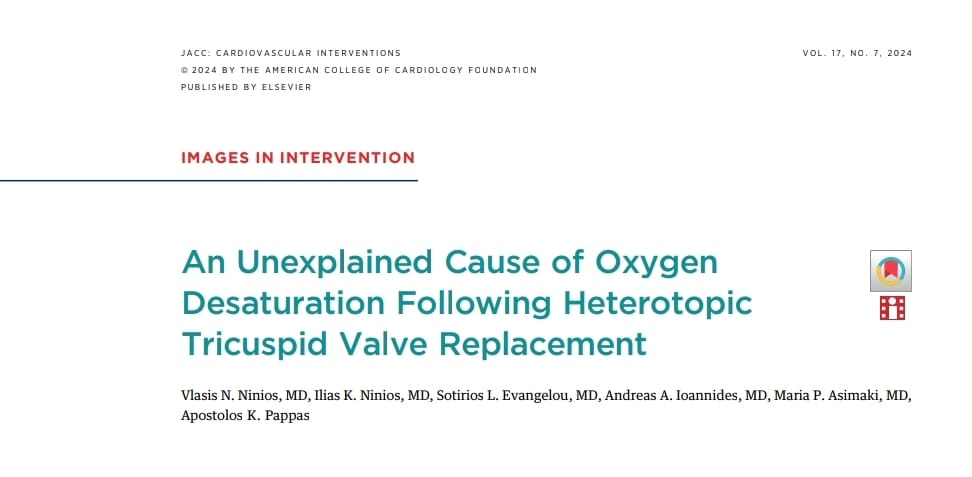
The procedure was uncomplicated and involved implanting a 25-mm valve in the superior vena cava and a 35-mm valve in the inferior vena cava (IVC). It was noted that the IVC valve was positioned relatively high (Figure 1) but resulted in a significant reduction in IVC pressure.
Post-procedure the patient demonstrated an improvement in heart failure symptoms and a reduction in diuretic requirement. At the 1-month follow-up, echocardiography confirmed the absence of valve migration and satisfactory valve function.
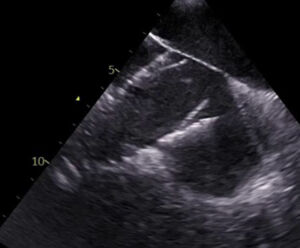
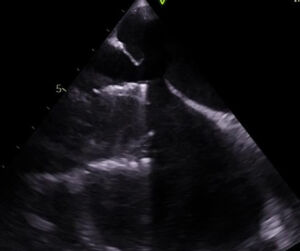
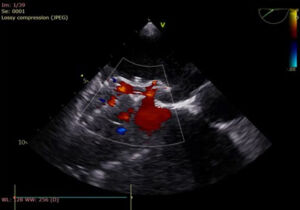
Approximately 2 months later, the patient presented with increased dyspnea and resting oxygen saturation levels between 80% and 82% that were unresponsive to diuretics. Investigations including pulmonary examination, chest X-ray, and computed tomography pulmonary angiography yielded normal results. However, a transesophageal echocardiogram revealed a new atrial septal defect (ASD) measuring 14 × 16 mm with right-to-left shunting (Figures 2 and 3, Video 1), likely secondary to late erosion of the atrial septum because of the proximity of the IVC valve.
The patient underwent successful percutaneous ASD closure via the right femoral vein. A 24-mm Amplatzer ASD occluder device (Abbott) was deployed through the IVC valve (Figures 4 and 5, Video 2). This resulted in an immediate increase in oxygen saturation to 95% with no residual shunting.

To our knowledge, this is the first case of late atrial septal erosion secondary to the proximity of the IVC portion of the TricValve. Unexplained oxygen desaturation should yield a high level of clinical suspicion. Percutaneous ASD closure through the IVC valve is a viable solution for such a complication without compromising the function of the TricValve.
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
Appendix
Video 1. Eroded Atrial Septum With Protrusion of the Valve Frame
Video 2. ASD Closure Device With No Residual Shunt